
Breaking the Obsessive-Compulsive Cycle: Your Key to Freedom from OCD
Written by: Allyson Inez Ford, MA, LPCC
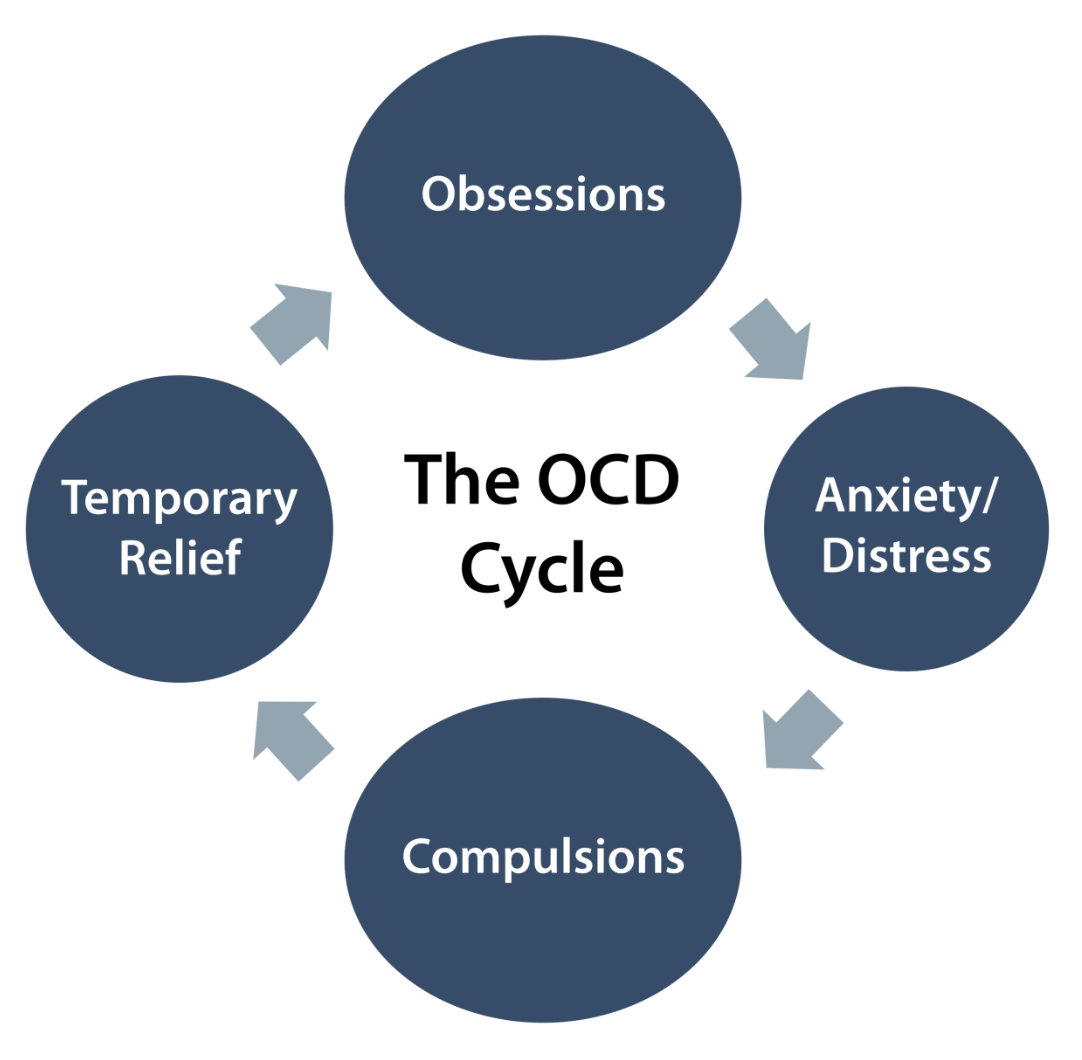
What is the obsessive-compulsive cycle?
Understanding the obsessive-compulsive cycle is a big part of finding relief from OCD. This cycle is what reinforces the intrusive thoughts and makes them anxiety provoking in the first place. Breaking the cycle isn’t easy, in fact it often feels totally paradoxical. When you feel anxious, it’s natural to want to do something to relieve the anxiety. However for people with OCD, this is where compulsions come in and unfortunately, the compulsions keep your brain scanning for a possible threat (aka- you’re probably going to feel very anxious!).
Let’s look at an example from a common OCD Theme:
For example: “I had the thought that I might have skin cancer and now I can’t stop worrying about it- I am scanning my body constantly to see if I can find any abnormal looking marks on my skin. I feel better when I don’t find any, but the fear continues to pop up and it’s consuming so much of my brain space. In addition to scanning my skin, I am now spending a lot of time researching signs and symptoms online. This makes me feel slightly better in the short term, but the fear doesn’t fully go away- I can’t seem to make it stop!” In this example, the person is suffering with a health anxiety subtype of OCD. Remember that there are many subtypes of OCD, be sure to learn about how your specific OCD manifests. For the purposes of highlighting how the O-C cycle plays out, we’ll use this health related OCD spiral.
Breaking down the cycle:
The obsession part of the cycle is the intrusive thought that drives the fear. In the example above, it’s the fear of having skin cancer.
The distress/anxiety is what the person feels after having the intrusive thought. Instead of being able to let the thought pass on by and just shrug it off, the person feels anxious and leans into the possibility that it could be true, despite having no real here and now evidence.
The compulsion is anything done to relieve the distress/anxiety from the intrusive thought. In this example, it’s the scanning of the skin for signs of skin cancer as well as researching online what signs and symptoms to look out for. Compulsions can be behavioral, mental (ruminating is a compulsion), reassurance seeking based or avoidance based.
The compulsion provides very short term relief, but at the same time, it sends the message to the brain that “this is something very important we need to keep paying attention to!” Thus, the cycle perpetuates and we find ourselves continually having the intrusive thoughts. Often times, as the thought keeps returning, the person becomes more and more anxious. Even more compulsions develop and the time spent on them usually increases. In the example above, the person might then ask family members repeatedly about their health histories, in an attempt to seek reassurance that cancer is not in their genetics.
Sound familiar? Keep reading!
Hard truth: we can’t change our thoughts
Research estimates we have around 70,000 thoughts a day. That is A LOT of thoughts. Non-OCD brains filter out intrusive thoughts quite easily, the seem to just pass on by and be disregarded because the person doesn’t pay much attention to them and isn’t anxious about them because they have a foundation of self trust that protects them from questioning who they are or what’s happening in their reality. You likely do this to a certain degree too- you have the ability! It’s just that OCD latches onto things that we are vulnerable to and triggers an anxiety response that makes us feel like the thought has merit. The hard part about this is, we can’t stop our thoughts from being there and we can’t choose which thoughts pop into our brain. If I were to tell you: “don’t think of a white elephant” you would have a hard time NOT thinking about it. When we try to push thoughts away or avoid them, they usually only get louder and that is very true for OCD. The only thing we can control is our response to the thoughts. We can choose how much attention we pay them, the meaning we make from them, the behaviors we do to try to control them and the way we treat ourselves when we have them. Those responses make all the difference in terms of whether or not the OCD gets louder or quieter.
Breaking the cycle
Since we can’t change the thoughts themselves, breaking the O-C cycle means we intervene at the compulsion part of the cycle. In Exposure Response Prevention therapy, we work on gradually reducing the compulsions we engage in while gradually facing our fears. Over time, our brain learns that a) when we face our fears without using a compulsion, over time anxiety decreases on its own and the thoughts get quieter (habituation effect) or b) we still feel the anxiety but we learn we can tolerate it without compulsions, the exposure teaches us a new lesson that overrides the original fear (we can have the intrusive thought and not doing anything about it, and the OCD fear either doesn't come true which disconfirms the belief that the compulsion keeps us safe- or the fear does come true and we cope with it) and we still get our life back from OCD (inhibitory learning).
Overall, breaking this cycle using ERP helps us learn that:
Intrusive fears are less probable or severe than predicted
Anxiety and intrusive thoughts themselves are safe and tolerable (anxiety naturally rises and falls on it’s own without any compulsion)
Compulsive rituals are not necessary for safety or to tolerate anxiety
This process takes time and practice, but when we break the obsessive compulsive cycle, we begin creating space from our OCD and gain more agency in how we want to show up in our lives. It might sound somewhat simple, but everyone’s OCD is unique and therapy requires some flexibility and creativity with this model.
It’s also important to note that ERP is not the only evidence based model for OCD, and not the only way to break the obsessive-compulsive cycle. Roughly 50% feel moderate relief from OCD with ERP, which is a lot of people, but it also leaves out a lot of people. For that other 50%, treatments like Inference-Based CBT (I-CBT) are also highly effective; I-CBT intervenes at the cognition part of the O-C cycle and does not require any exposure. This model can feel more tolerable for some sufferers, especially neurodivergent folks (there is some research that indicates less habituation effect for autistic brains- though there are ways to adapt ERP for autistic folks, too).
At ED and OCD Therapy, we are trained in both models and will work with you to find what fits for your specific experience of OCD. As a person with lived experience of OCD, I can tell you that both of these models have been helpful for me! I don’t believe there is a “better” or “worse” -they are just vastly different since they intervene at different points of the OCD cycle.

Final Thoughts
It is possible to learn to live a full life with OCD. It’s possible to find relief from the constant barrage of intrusive thoughts and compulsions. Your brain is capable of learning safety and learning to trust yourself. You already do it in other areas of your life! Together, we can help you build self trust even in the midst of an OCD spiral- so that you can see the cycle and not engage. We want to help you get your life back from OCD, please reach out if this resonates for you! We offer free 15 minute phone consultations to make sure we are a good fit, we are also happy to provide referrals for other trusted colleagues if you don’t click with us.